
For at least one transition of care or referral, the MIPS eligible clinician that transitions or refers their patient to another setting of care or health care provider — (1) creates a summary of care record using certified electronic health record technology (CEHRT); and (2) electronically exchanges the summary of care record.
Measure Overview
Objective: Health Information Exchange
Measure: For at least one transition of care or referral, the MIPS eligible clinician that transitions or refers their patient to another setting of care or health care provider — (1) creates a summary of care record using certified electronic health record technology (CEHRT); and (2) electronically exchanges the summary of care record.
Measure ID: PI_HIE_1
Exclusion: Any MIPS eligible clinician who transfers a patient to another setting or refers a patient fewer than 100 times during the performance period.
Exclusion ID: PI_LVOTC_1
Definitions of Terms
– Patient name
– Demographic information (preferred language, sex, race, ethnicity, date of birth)
– Smoking status
– Current problem list (eligible clinicians may also include historical problems at
their discretion)*
– Current medication list*
– Current medication allergy list*
– Laboratory test(s)
– Laboratory value(s)/result(s)
– Vital signs (height, weight, blood pressure, BMI)
– Procedures
– Care team member(s) (including the primary care provider of record and any additional known care team members beyond the referring or transitioning clinician and the receiving clinician)
– Immunizations
– Unique device identifier(s) for a patient’s implantable device(s)
– Care plan, including goals, health concerns, and assessment and plan of treatment
Referring or transitioning clinician’s name and office contact information
Encounter diagnosis
– Functional status, including activities of daily living, cognitive and disability status
Reason for referral
*Note: A MIPS eligible clinician must verify that the fields for current problem list, current medication list, and current medication allergy list are not blank and include the most recent information known by the MIPS eligible clinician as of the time of generating the summary of care document or include a notation of no current problem, medication and/or medication allergies.
Measure Reporting
Numerator/Denominator
Numerator: The number of transitions of care and referrals in the denominator where a summary of care record was created using CEHRT and exchanged electronically.
Denominator: Number of transitions of care and referrals during the performance period for which the MIPS eligible clinician was the transferring or referring clinician.
Measure Scoring
- Required for Promoting Interoperability Performance Category Score: Yes, unless submitting the alternative, HIE Bi-Directional Exchange measure (HIE_5)
- Measure Score: 20 points
- Eligible for Bonus Score: No
Note: In order to earn a score greater than zero for the Promoting Interoperability performance category, MIPS eligible clinicians must:
- Complete the activities required by the Security Risk Analysis and High Priority Practices SAFER Guide, submit their complete numerator and denominator or Yes/No data for all required measures, and attest to the Actions to limit or restrict compatibility or interoperability of CEHRT statement.
- Failure to report at least a “1” in all required measures with a numerator or reporting a “No” for a Yes/No response measure (except for the SAFER Guides measure2) will result in a total score of 0 points for the Promoting Interoperability performance category.
Freedom | EHR Workflow
MIPS Conformance Calculation
Denominator: Number of transitions of care and/or referrals made during the performance reporting period.
Numerator: Number of transitions of care and/or referrals during the performance period where a summary of care record was created and provided electronically to the provider to which you are referring the patient.
How To:
Step 1: Create a new consult/referral order.
From the Consult > Order Detail tab, at a minimum fill in the highlighted fields and click SAVE.
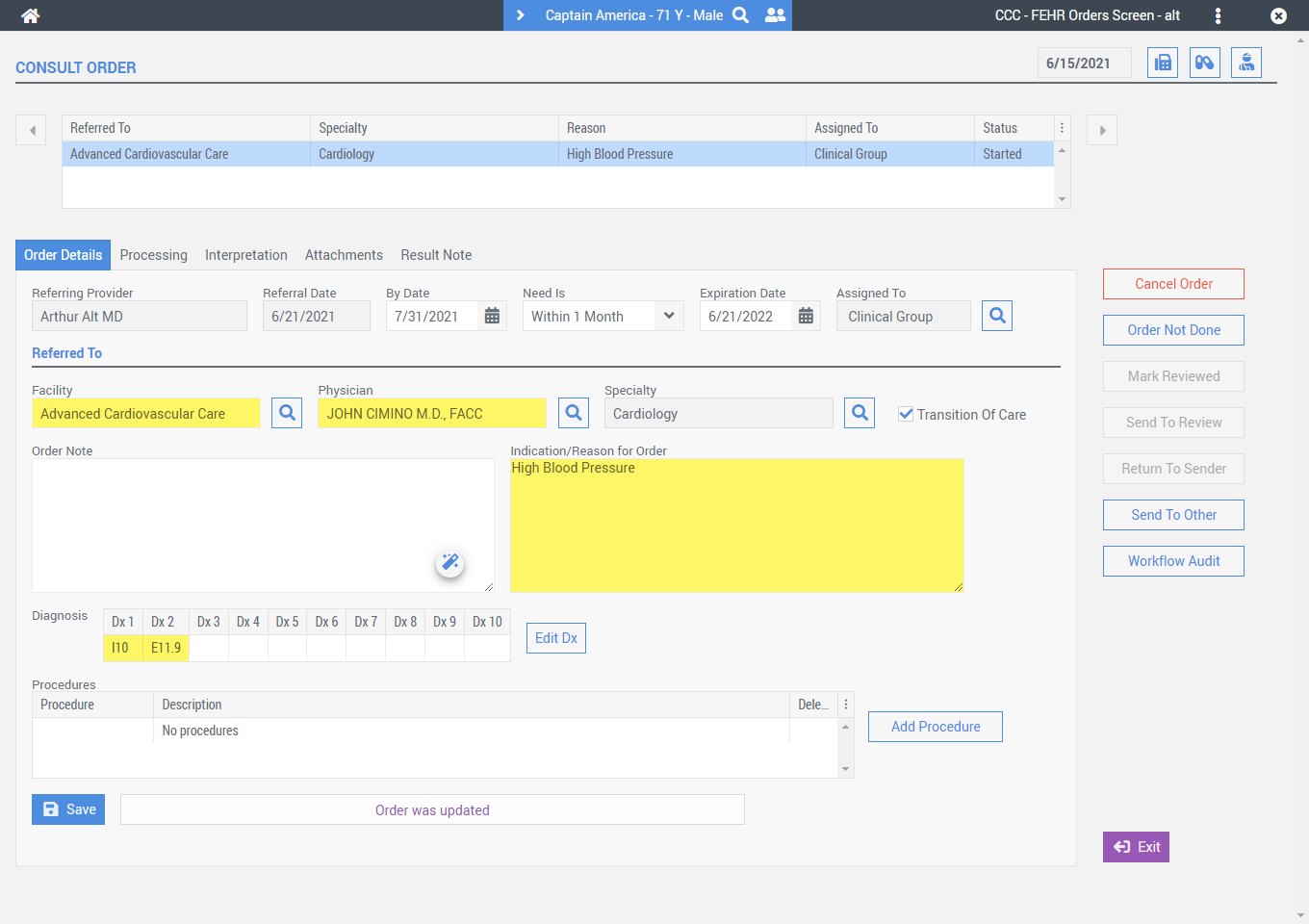
Facility – The Facility field is used to indicate the clinic/organization you are referring the patient to.
Physician – The Physician field can be used to indicate a particular physician at the facility you would like the patient to see.
This referral is a transition of care – is checked by default when creating a new consult/referral order(s).
Indication/Reason for Order – is used to indicate the reason for the consult/referral order. However, in the event that the Indication/Reason for Order comment is left blank, Freedom | EHR will look for a diagnosis code description or procedure code description associated with the consult order and use these in its absence.
Step 2: Complete the processing of the new consult/referral order.
Within the Consult > Processing tab, continue filling in any necessary information and then select the Consult Confirmed button.
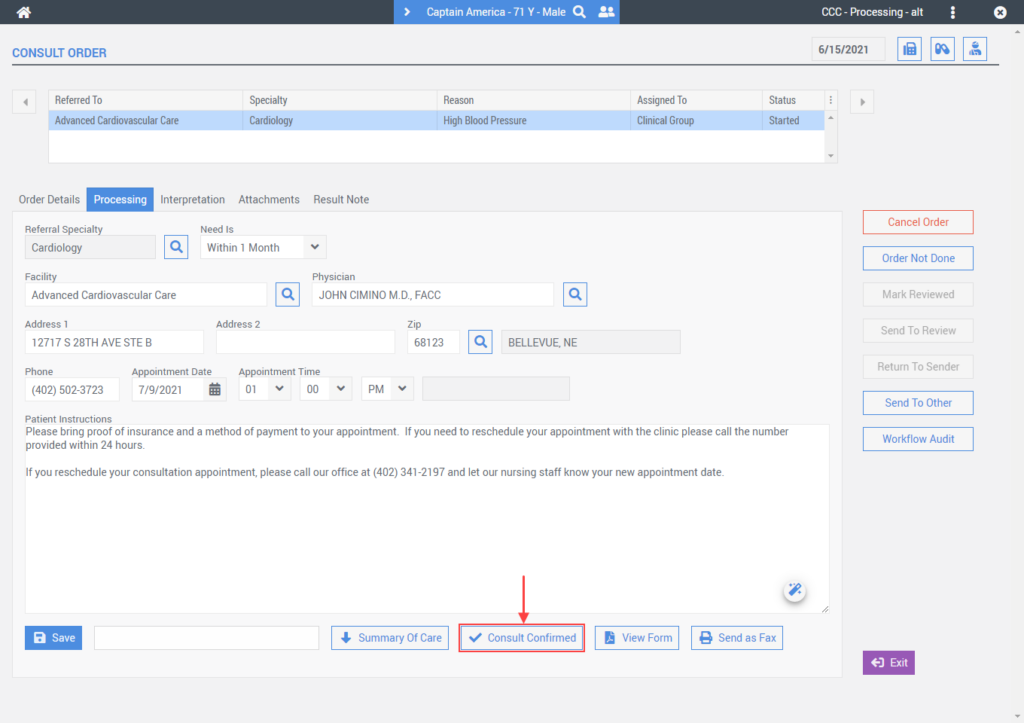
When you use a Facility that has a direct address associated with it, Freedom | EHR will automatically create the Summary of Care Record and transmit it electronically via the direct messaging standard.
Following this workflow will ensure Freedom | EHR creates the Transition Out of Care record and indicates that health information exchange was sent electronically for MIPS numerator credit.
Data Validation
CMS will publish guidance to help clinicians better understand the supporting documentation they should retain when attesting to the MIPS requirements. CMS calls this guidance “MIPS Data Validation Criteria” as it outlines the types of documentation that should be retained to validate the data the provider submits to CMS at the end of the performance period. You must keep documentation for six years subsequent to submission. We suggest reviewing this validation document to ensure you document your work appropriately.